When you’re deep in recovery, the terms slip and relapse often swirl in conversations, therapy sessions, and support groups. Though they may seem similar, understanding the difference between a slip and a relapse is vital for anyone navigating sobriety. This isn’t just semantics—it’s about recognizing where you are in your journey, responding appropriately, and staying on track toward long-term healing.
What Is a Slip (aka Lapse)?
A slip can be:
- A one‑time or very short event,
- Unplanned or impulsive,
- Quickly followed by addiction‑recovery behaviors, such as reaching out to a support system.
For example:
- Taking a single sip of alcohol at a wedding by accident.
- Accepting a pill thinking it was harmless.
- Feeling overwhelmed, using once, then returning to your recovery routine.
Support groups and clinical literature describe it as a brief deviation, not destruction.
Key characteristics of a slip:
- Single, isolated instance
- Immediate regret/guilt
- Return to recovery behaviors (therapy, meetings, sponsor outreach)
- Not a conscious abandoning of sobriety
What Is a Relapse?
A relapse, by contrast, is more serious:
- It often involves premeditation—buying, planning, consuming repeatedly.
- It tends to be prolonged, erasing progress made in sobriety.
- It reflects a breakdown in coping strategies and a full return to addictive behaviors.
Statistics underscore its prevalence: between 40% to 60% of people in recovery experience a full relapse during their early sobriety years. Recovery centers echo that a relapse often indicates the need for more intensive treatment support.
Core features of relapse:
- Repeated use – bingeing or sustained usage.
- Premeditation and planning – not impulsive.
- Abandoning recovery plan – no meetings, no therapy, lost structure.
- May require detox or inpatient treatment to get back on track.
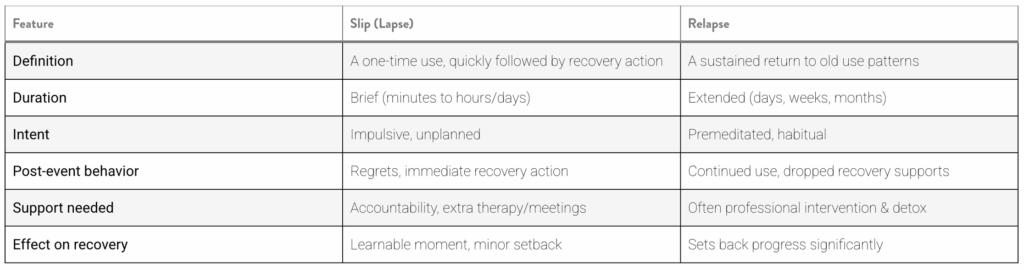
Side-by-Side Comparison
Why This Distinction Matters
1. Mental Framing & Self-Compassion
- Identifying a slip helps avoid catastrophizing. It’s a chance to learn, not a reason to quit recovery.
- Mislabeling a slip as a relapse can trigger guilt and feelings of failure, increasing risk of real relapse.
2. Appropriate Response
- A slip calls for boosted support: journaling, therapy, meeting attendance.
- A relapse may require medical detox, a change in treatment plan, or residential stay.
3. Preventing Escalation
- Early recognition of a slip allows for immediate intervention. That’s why relapse prevention models stress identifying warning signs—like stress, triggers, denial, and cravings.
The Recovery Continuum: Emotional → Mental → Physical
Cognitive-behavioral relapse-prevention frameworks spell out a three-phase descent:
- Emotional relapse – internal stress, poor self-care, unaddressed feelings.
- Mental relapse – internal conflict, thoughts about substance use, fantasizing.
- Physical relapse – actual substance use, potentially progressing to a slip and beyond.
Understanding this helps catch warning signs before a physical relapse occurs.
Common Triggers for Slips and Relapses
Research and recovery communities identify key triggers:
- Stress – job loss, relationship conflict, grief
- Social pressure – parties, triggers in the community
- Mental health issues – untreated depression/anxiety
- Environmental cues – places or objects tied to past use
- Celebratory drinking – “just one won’t hurt” mindset
- Lack of support or self-care routine
What to Do After a Slip
- Acknowledge it – name it a slip, not a failure.
- Avoid shame – self-compassion fuels recovery. Shame can backfire.
- Analyze triggers – identify what led to it: stress, social, thought patterns.
- Recommit to recovery – schedule extra meetings and support sessions.
- Adjust your plan – update relapse prevention strategies and coping skills.
- Communicate with your support circle – be open to accountability.
Responding to a Relapse
- Admit it fully – hiding a full relapse only deepens its consequences.
- Seek professional help – outpatient, residential, medication-assisted treatment may be necessary.
- Revise the treatment plan – include new coping skills, mental health care.
- Build or enhance support networks – sponsors, peer groups, counseling, family therapy.
Sobriety Is a Process, Not a Final State
As Kelly Osbourne reminded us, relapse isn’t failure—it’s a sign your current plan wasn’t enough. Relapse is part of recovery – not a permanent endpoint.
At Elevate Recovery Homes, we understand that transitioning back into daily life is a pivotal point in treatment. Our sober living homes for men provide a structured, supportive environment—bridging the gap between inpatient rehab and full independence.
What makes our sober living special:
- Peer-driven accountability – residents live together, share responsibilities, and support each other.
- Recovery-focused structure – regular house meetings, chores, and curfews keep daily life orderly.
- Access to therapy and meetings – we work with local outpatient providers and 12-step/alternative recovery groups.
- Trigger-free environment – roommates are in recovery, and no substances are allowed on premises.
- Life skills coaching – budgeting, job searching, managing stress, building healthy routines.
By staying with us, men gain real-world experience in a safe setting, reinforcing habits that keep slips from turning into relapses. We don’t just “maintain.” We elevate each person’s potential.